Acute Medicine induction booklet was contributed by the following;
written by Dr Tamar Saeed
Select the booklet titles below to expand the table to view more information.
Acute Medicine Introduction
ACUTE INTERNAL MEDICINE COVERS THE FOLLOWING AREAS:
- AMU 1 (Rainbow unit ground floor)
- AMU 2 (Rainbow unit first floor)
- AMU 3 (A4 ward)
- AMU Assessment area
- ED
- SDEC (Same Day Emergency Care)
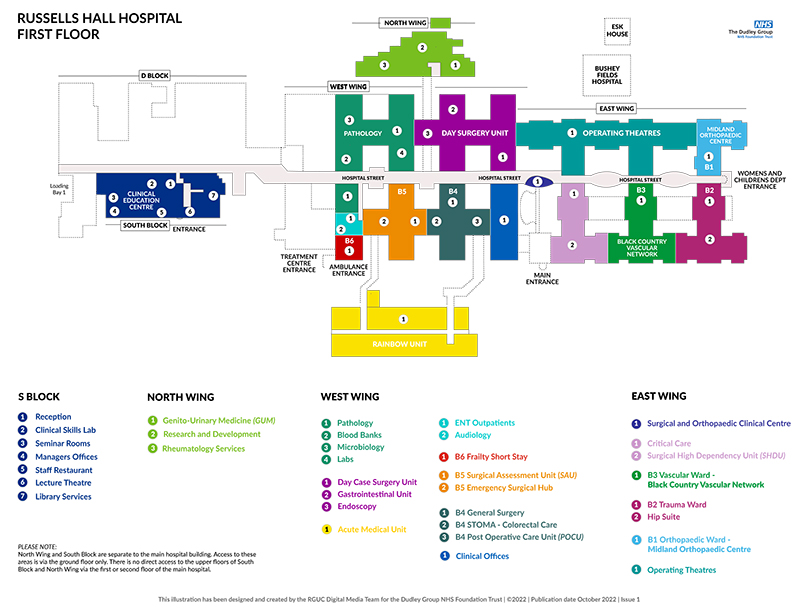
View the location of the Acute Medicine areas on our hospital maps.

RAINBOW UNIT
AMU 1 (Rainbow unit ground floor)
- 30 beds including 8 monitored beds
- 2 Teams (AMU 1 A and AMU 1 B)
- AMU 1 A – beds 1- 11 and monitored beds 1 – 4
- AMU 1B – beds 12-22 and monitored beds 5 – 8
AMU 2 (Rainbow unit first floor)
AMU 2 A and AMU 2 B
- AMU 2 A beds 1- 12 and side room 28-30
- AMU 2 B beds 13- 24 and side rooms 25 – 27
Each 15 beds station has a consultant and at least 2 residents (3 at times)

AMU ASSESSMENT AREA AND ED (08:00-16:00)
- 22 beds assessment area next to ED
- Medical patients transferred for assessment also clerked in assessment area
- Three acute medicine teams
- Two teams in assessment area
- One team sees 10 patients and the other team sees 12 patients
- One team (post take team) in ED to post take the night patients
A4 WARD
AMU 3
- 12 beds on the ward
- 1 junior does WR with consultant and/or registrar
- Shift 08:00 – 16:00

SDEC (Same Day Emergency Care)
- Mobile patients who are likely to be discharged the same day
- Your job is to clerk patients, post take with consultants and registrars and review old scans
- The names are on the whiteboard, write your name next to the patient you ‘pick up’
- High pressure area
- Ensure you take appropriate breaks and attend any teaching arranged
- Departmental doppler US facility available
Acute Medicine Team
Consultants and other Team staff
| Consultant | Secretary | Extension |
|---|---|---|
|
Dr Patha Nandi |
Donna Swindells |
3141 |
|
Dr Ibrahim Malik |
Heather Kearns |
3141 |
|
Dr Murali Veerabahu |
Heather Kearns |
3141 |
|
Dr Tamar Saeed |
Heather Kearns |
3141 |
|
Dr Athanasios Georgalas |
Lauren Robins / Danielle Greenhill |
3141 |
|
Dr Ragunath Durairajan |
Lauren Robins / Danielle Greenhill |
3141 |
|
Dr Randa Abasaeed-Elhag |
Lauren Robins / Danielle Greenhill |
3141 |
|
Dr Snigdhendu Mandal |
Lauren Robins / Danielle Greenhill |
3141 |
|
Dr Anirban Chakraborty |
Donna Swindells |
3141 |
|
Dr Alyson McClung |
Donna Swindells |
3141 |
|
Dr Ahmad Elsharkawi |
Heather Kearns |
3141 |
|
Dr Faisal Butt |
Lauren Robins / Danielle Greenhill |
3141 |
|
Dr Gautam Bagchi |
Heather Kearns |
3141 |
|
Dr Tarunya Vedutla |
Heather Kearns |
3141 |
|
Dr Vikram Anumakonda |
Donna Swindells |
3141 |
| Other Staff | Position |
|---|---|
|
Victoria Mellor |
Rota Manager |
|
Vick Smith |
Rota Manager |
|
Stacie Grae |
Rota Manager |
|
Clare Weatherstone |
Matron |
Acute Medicine - Types of Shifts and On Call Teams
AMU Ward Round Shifts (08:00-16:00)
- The ward round starts at 8.00 with the consultant.
- Let the night clerking team post take their patients first.
- As there are two residents per ward round, one write the list, one write in the notes.
- Try to type the round as you go along.
- If the consultant agrees, jobs can be done during the ward round.
- From 15:30 the ‘handover’ doctor will start: PLEASE NOTE discharge letters and jobs that could have been done during the day should not be handed over.
Shift patterns in SDEC (Weekdays)
- Hot clinic 08:00 – 16:00 reg
- SDEC returns 08:00 – 16:00 reg
- SDEC Reg 08:00 – 16:00
- SDEC Reg 12:00 – 22:00
- SDEC 08:00 – 16:00 (2 residents)
- SDEC 08:00 – 20:00 (2 Pas)
- SDEC 14:00 – 22:00 (approx 4 residents)
- SDEC handover 16:00 – 00:00
- SDEC ACP 08:00 – 21:00
Shift patterns in SDEC (Weekends)
- Reg 08:00 – 16:00
- SHO/ACP 08:00 – 20:00
- SHO 09:00 – 21:00
- SHO 13:00 – 21:00
Handover Shift (15:30 - 21:30)
- Attend the AMU1 doctors office at the start of the shift
- The day team medical team will handover their jobs to you
- Nurses/doctors will also put the jobs on Nerve Centre
- Pick up the ‘Nerve device’ from the site coordinators office next to the hospital entrance.
- You are not responsible for clerking new patients but you will have to look after existing patients that have been handed over to you.
- You can hand over outstanding jobs to the AMU night doctor before you leave
- Handover at the acute medicine seminar room should be attended at 21:00
Handover and Huddle
- Everyday 09:00 and 21:00 in the AMU seminar room
- Led by medical registrar
- All medical staff, Hospital@Night, outreach
- Ensure collection of Nerve Centre and bleeps
Medical Registrars
- There are two registrars –
- 1st Reg covers the medical take and ground floor areas (ED, AMU and assessment area)
- 2nd Reg covers the rest of the wards including MECU
- Clearly, the registrars can mix skill sets and if one is busy on MECU, I would expect the other to attend the stroke alert for a potential thrombolysis for example.
- It is important to meet and ‘huddle’ to assess workload.

The Rota
- Medirota
- Hub → Links → E-rostering → Medirota
- Login
User name: gim@dgft.com
Password: Dudley01
Handover and Hospital at Night
- AMU seminar room 09:00 and 21:00 for 30 minutes
- Follows RCP handover guidelines
- Confirms MET team
- Check staffing – who is working and where
- H@N – ANP support
- Weekdays 17:00 – 09:00
- Weekends 24/7
On Call team
Weekdays Day Team
- Registrar front door 09:00 – 21:30
- Registrar ward cover 09:00 – 21:30 (to cover own speciality 09:00-17:00)
- GIM front door clerking SHO 1 (bleep 1015) 09:00-21:30
- GIM front door clerking SHO 2 (bleep 6011) 09:00 – 21:30
- SHO front door clerking without bleep 09:00 – 21:30
- F1 clerking 09:00-17:00 (bleep 6010)
- Two AMU SHO for clerking 09:00-21:30
- SHO Long day ward cover (09:00-17:00 covering own ward and 17:00-21:30 covering wards as on call)
- F1 own specialty 09:00-17:00
- F1 ward cover 17:00-21:30
Weekends Team
- Registrar front door – 09:00-21:30
- Registrar ward cover – 09:00 – 21:30
- GIM front door clerking SHO 1 (bleep 1015) 09:00-21:30
- GIM front door clerking SHO 2 (bleep 6011) 09:00 – 21:30
- SHO front door clerking without bleep 09:00 – 21:30
- Two AMU SHO for clerking – 09:00 – 15:30, 15:30 – 21:30 will go to AMU / assessment area handover (one each)
- F1 clerking 09:00-17:00 (bleep 6010)
- SHO long day ward cover (09:00-17:00 covering own ward and 17:00-21:30 covering wards as on call)
- FY1 long day ward cover (09:00-17:00 covering own ward and 17:00-21:30 covering wards as on call)
Night Shift
- Front door reg 21:00 – 09:30
- Front door night SHO 1 (21:00 – 09:30) – with bleep (1015)
- Front door night SHO 2 (21:00 – 09:30) – without bleep
- Front door night SHO 3 (21:00 – 09:30) – without bleep
- 1 AMU SHO (to cover AMU and/or clerking)
- 1 AMU SHO (to cover AMU assessment and A4)
- Ward cover registrar 21:00 – 09:30
- Ward cover SHO (21:00 – 09:30) with bleep 6011
- FY1 medicine wards (21:00 – 09:30)
Acute Medicine - VTE in SDEC

- Clerk patient and include a Well’s score, and a D-dimer in your decision-making process.
- If consultant agrees that we must rule out a DVT.
- Request scan on Sunrise.
- Organise scan. Today or book for tomorrow/ next day. Speak to Corinna / Mostafa / Gladys. Give an appointment.
- If patient is waiting until the following day, need to give a STAT treatment dose of Enoxaparin.
- Complete TTO. Give hospital pink prescription.
- Liaise with nursing staff.
If result is positive - i.e this is a DVT
- A referral to anticoagulation needs to be made on Sunrise.
- SDEC review letter / summary of admission (found on Sunrise – enter documents).
- They will need to be given a pink prescription for rivaroxaban (check creatinine clearance)
- The prescription only needs to be for 21 days
- If they have cancer – consider enoxaparin, if they are pregnant / bleeding risk, discuss with consultant whether to split dose.
if negative
- SDEC review letter / summary of admission
- Consider alternative diagnoses
- You can often book a CTPA for the following day – SDEC have daily slots – but double check this with the nurse in charge of SDEC.
- There is a PE diary/schedular.
- For young females go for V/Q scan but remember patients must have a clear CXR and no respiratory disease.
- Give a dose of Enoxaparine if patient has a scan the following day / if after the weekend will need a pink prescription to take home.
- If the patient is UNSTABLE you will need to arrange an URGENT CTPA.
If result is positive - similar management to DVT
- SDEC review letter/summary of admission
- Anticoagulation referral on sunrise
- Enoxaparin/other anticoagulation prescription for 21 days
- Ensure checklist completed.
if negative
- VTE letter to be completed and management will be guided towards an alternative pathology.

Acute Medicine - Further Information
Medical Clerking
- Now electronic
- Drug list and chart. Get an SCR
- VTE assessment – we use Enoxaparin
- Discharge Letter
- Please state the name of the discharging consultant on the discharge letter
- This may be different to that stated on Sunrise
Critical Care Referrals
- Critical Care referrals should be made to the Critical Care Resident on bleep 6012
- Patients who do not need ITU care but require level 1 care should be referred to MECU (Needs to be discussed with MECU consultants or out- of-hours with the GIM consultant on call).
- For NIV discuss with a respiratory consultant on call (patients can be transferred to C5, CCU or MECU for NIV).
Specialty Input
- There is lots of specialty support available
- Methods vary and we no longer use FAX
- There is variability in the referral methods, with some using emails, phone, bleep or Sunrise. Make sure you use the correct one.

Imaging
- Imaging requests are prioritised depending on their urgency & details on the form
- If urgent d/w radiology consultant or registrar is best and consultant to Consultant if needed or imaging delayed
- Write a good request with key points e.g. CT head – head injury, anticoagulated, to exclude traumatic brain injury
- Radiology online – out of hours (Reg or above needs to discuss)
Discharge letter
- Aim for a high quality – see Acute Medicine Induction booklet
- State name of discharging consultant
- Think GREAT –
- G for GSF Code, R for Resuscitation Status, E for End of Life Care Medication, A for Advance Care Planning, T for Treatment Escalation Plan
- Include important information regarding changes to feeding regimes so that nursing homes can be updated.
Breaks
Resident doctors must receive:
- at least one 30-minute paid break for a shift rostered to last more than 4.5 hours.
- a second 30-minute paid break for a shift rostered to last more than 9 hours.
The breaks can be taken flexibly during the shift, and should be evenly spaced where possible.
These would normally be taken separately but may if necessary be combined into one longer break.
Abscence
Call the station / registrar / consultant you are working with that day (if on call the call the on call registrar/consultant)
AND
Email the generic email, medical workforce and your supervisor
Messages left to staff outside this process will not be accepted.
Health and Wellbeing
Staff that are happy and thriving in their working environment will inevitably have a more enjoyable experience in the workplace, contributing to the provision of excellent health care for all of our patients. The Dudley Group recognises our commitment to staff wellbeing in a variety of ways.
Select the link below to find out more how the Trust can support you.