Psychiatry induction booklet was contributed by the following;
written by Dr Iona Gordon, Dr Lena Hussain & Dr Noreena Syed
Reviewed by Dr Praveen Kumar
Updated by Dr Gbemi Arolasafe
Select the booklet titles below to expand the table to view more information.
Psychiatry Ward Timetables
There are three different FY1 Psychiatry jobs so timetable is dependent on your job allocation.
- FY1 for Old Age Psychiatry
- FY1 for General Adult Psychiatry
- FY1 for Early Intervention in Psychosis Psychiatry
Example Timetable for Old Age Psychiatry
| Day | Monday | Tuesday | Wednesday | Thursday | Friday |
|---|---|---|---|---|---|
|
AM |
Ward work |
Ward round |
Ward work 10:00 MDT |
Ward round |
10:00 Baliant and Teaching |
|
PM |
Ward work |
Ward work |
Ward work |
Supervision |
Ward work |
Old Age Psychiatry Team
Dr S Abilash – Consultant
Dr D Kamal – Middle grade
Also in team:
SHOs consisting of: FY2s, core and GP trainees
Elisha Hall – Secretary
Example Timetable for General Adult Psychiatry
| Day | Monday | Tuesday | Wednesday | Thursday | Friday |
|---|---|---|---|---|---|
|
AM |
Ward work and OP Clinic |
10:00 FY1 Teaching (ward review) |
09:00 MHAS |
09:00 Ward work |
10:00 Baliant and Teaching |
|
PM |
Ward work |
Ward work |
MHAS |
Ward work |
Ward work |
General Adult Psychiatry Team
Dr Hullamane – Consultant
Dr R Byra-Reddy – Middle gradeDr Nay Aung – Clinical fellow / CSW
Also in team:
SHOs consisting of: FY2, core and GP trainees
Donna Ross – Secretary
| Day | Monday | Tuesday | Wednesday | Thursday | Friday |
|---|---|---|---|---|---|
|
AM |
09:30 Zoning |
10:00 FY1 Teaching |
09:30 Zoning |
09:30 Zoning |
10:00 Balint & lunchtime teaching (on MS teams) |
|
PM |
Dr Shankar Clinic |
Dr Ravi Clinic |
|
Impatient ward round at Bushey Fields |
Administration afternoon |
Early Intervention Team
Dr Ravi – Consultant
Dr D Kamal – Associate Specialist
Also in team:
CPNS, social workers, psychologists, secretaries and students
General Timetable
There is one on-call doctor who is FY2 or above designated as the duty doctor for a day/night shift. FY1s are not required for this due to provisional registration with the GMC preventing the ability to section patients, so dealing with new admissions or any psychiatric emergencies would be difficult.
On call rotas as per GIM medicine rota that requires you to cover various on-call shifts at RHH. You are entitled to timetabled days off depending on your on-call commitments – let your secretary and SHO know when you are due to be off and someone will cross-cover for you.
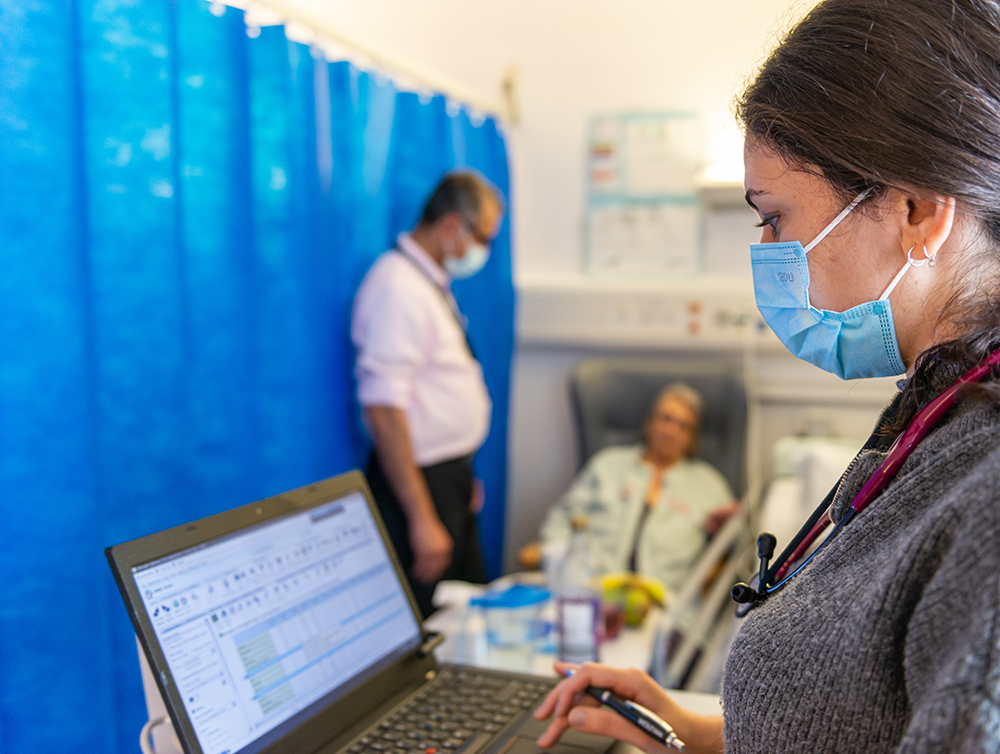
Notes:
Notes are now on a system called RiO which you may have used during medical school. This enables you to see all medical and nursing notes for a patient for both OP and IP contact, as well as any letters and/or other documentation. You will need to complete RiO training in order to obtain your log in details so get this done over induction otherwise you won’t be able to do any documentation.
Old Age Psychiatry Ward
Ward Round
Ward rounds are called ward reviews and they happen once a week in each ward in the review room with allied HCPs often present (such as OT, Psychologists, Care Coordinators and Social Workers). The nursing team will take the notes and drug charts into the clinic room. There should be a ward review proforma on RiO (or one to upload into the progress notes). Go through each heading of this and try to fill it out from the consultant-led discussion of the patient. Nurses often leave a short review in notes prior to the ward review to get a basic understanding of how the patient has been doing but if not they will tell the group how the patient has been so you can make note briefly. Document observation levels and medication review (even if there are no changes). Seek senior medical help during the ward review if unclear.
New admission: for your consultant
We have to fill out all the clerking sheets in the patient’s folder:
- checklist
- patient alert
- admission booklet
- cardio-metabolic form
- VTE risk assessment
- capacity assessment form
- learning disability form
- cognitive assessment form
- care cluster
Do an ECG on every admission and general physical observations.
Fill out the drug chart using the GP summary letter or their own medications they bring in – the ward pharmacist will help you.
Control drugs have a separate form, as do the covert medication which needs to be signed by a consultant too.
Admission booklets are still done on paper and uploaded to RiO but all the others are done on RiO.

Discharges
TTOs are done when the patient is discharged from the ward. Ask the ward clerk for the TTOs if the nurses haven’t already given you them. General practice is to supply 14 days’ worth of TTOs at any one time but if the patient is at risk of an overdose pharmacy or the consultant advice may be to supply only 7 days.
When a patient has been discharged, first fill out a discharge notification letter available on the ward on or before the day of discharge along with their medication. After this you can start to fill in the discharge letter – as all the patient notes should be on RiO then it’s unlikely that you will need paper notes but they should be available in your pigeonhole in the secretaries’ office in Henry Lautch so you can check medication etc. You will be emailed a proforma to fill out as each consultant likes their discharges done a certain way. Older Adult discharge summaries tend to be shorter than the other sub-specialties as a whole.

Bleep
Whenever you get a bleep, (#1923 is Malvern and #1549 is Holyrood) ask if it is a job for one of your patients first so the nurses are aware of your specific role – if the other doctors are away then you can help out but primarily you are responsible for your patients only. If you haven’t received any bleeps for jobs, you can check the Doctors’ diary which is in the nurse’s office on Malvern and Holyrood. Check these in the morning as nurses tend not to bleep you until the jobs in the diary haven’t been done at around 4pm each day. Cross off the jobs when they’re done and let a nurse know it has been done if possible, for completeness.
When post-taking with a consultant you should present a brief history of what the patient came in with, their background and your assessment. You can then expect them to see the patient themselves with you.
After the consultant assessment, they will give you the likely diagnosis/differentials and finalise a management plan. This will be automatically marked on the list.
Patient observation levels
When deciding on observation levels (this is how much the nurses should interact with the patient depending on their risk).
- Level 1: general observations on the ward
- Level 2: nurses to check patients every 15min
- Level 3: at least one nurse to be at arm’s length away at all time.
- Level 4: two nurses to be at arm’s length away.
These needs reviewing daily but minimally at least every ward review. Don’t feel pressured to move observation levels up or down
The safety of patient and nurses’ input is valuable in deciding. Seek senior medical input if unsure about reducing observation levels. For those on level 2 observation or above, there is a daily form to be signed to monitor observations in front of the review sheets.
When you’re ready, it’s time to pick up the next patient to clerk and the cycle starts again! Don’t start on a new patient after 16:00 (if you are finishing at 17:00). If you are free/spare at end of shift, help others clerking with their jobs. As an FY1 you are not expected to clerk huge numbers of patients – 2 to 4 a day is fine, be comfortable in your practice.
Skills
Psychiatry is generally limited in what you can do so medications cannot be given IV as in the general hospital. There is a limited supply of oxygen available on the wards for emergencies.
To do bloods: phlebotomists come every Tuesday and Thursday so you can leave blood forms in the phlebotomy diary. Or you can do it yourself in the clinic room – sign and date by hand with stickers attached to form and bottles. Blood bags and blood forms are found in the labelled filing cabinets in the ward office. If after 5pm, the porter may not come so make nursing staff aware that someone will have to take the blood collected to RHH.
Radiology
Xray forms or radiology: When the forms have been picked up by the porter, you would have to chase X-ray/MRI/CT via switchboard to make sure the forms are entered onto Sunrise. For MRI/CT you would have to speak to the radiology registrar on duty to vet the request. After, you would call MRI/CT to update them and get an appointment for the patient.
The above process is similar for DaT scans, except you would need to speak to Dr Wong (consultant radiologist) to approve the request and ask the porter to deliver the request form to nuclear medicine to be entered onto Sunrise.

Bloods
To check blood results/cultures and radiology results: log in to the computer and then into CliniSys ICE. To get access to ICE, you need to fill a form to request access; this form can be found on the intranet. After logging in, go to Home > Patients > Search > Patient identifier (Name, NHS No, etc) > Search > Patient’s name > view patient’s report. Usually, blood results come within a day, and a paper form will come later which the ward clerk will put in the doctor’s diary book for you to sign. It’s best to upload a summary of the results to RiO as the nurses don’t have access to emis and put an impression/plan for the results as well. The nurses are mental health specialists so may struggle to interpret blood results.
Referrals
To make referrals to RHH: ring switch board (#0 on white phone) and ask for the secretary or medical/surgical reg depending on the issue. You can either refer via phone call or take their email address and do it this way. It is better for our patients if the team come here due to their risk, if possible. Then just document in notes your conversation as you would in any other notes.
Annual leave
Collect the form from post graduate centre in Henry Lautch and put your dates on and then ask the other junior doctors in old age psych to cover you on these dates. Try and get your requests in early if possible (6 weeks’ notice). Make sure you get your consultant to sign it too and return to Post graduate centre.
Rowans
Rowans (near Holyrood) is the mess for psych doctors. It’s nice to spend time together here for your lunch and breaks. You can work here too until your bleeped for jobs. There is also a prayer room you can use in Rowans or in Henry Lautch. In the Henry Lautch there is a junior doctor office which has computers you can use.
General Adult Psychiatry Ward
Ward Round
On Monday mornings, Dr Hullamane’s patients are seen across three wards – Clee (female ward), Clent (male ward) and Wrekin (mixed ward).
You must gather the patient’s notes, drug charts and find out from the nursing team how the patient has been over the weekend. You can find designated ward round proforma on Rio under Riverview which should have been partially filled in by the nurses on that day or the day before and be sure to fill in the Mental State Exam section and note any medication changes. If patients need Section 17 leave forms (blue), you can find these in the top drawer of the filing cabinet in the main office.

Discharging Patients
When a patient is discharged, you must complete a brief handwritten discharge proforma (white form with orange boxes – found in the filing cabinet) which is sent to the patient’s
GP on the same day of discharge to inform them briefly about the inpatient admission.
You must also handwrite the medications/TTOs on the back of the inpatient drug chart and send this to the pharmacy at RHH straight away. After a few days, if you check your pigeonhole (on the second floor next to the clinical offices), you’ll see the patient’s file there. Once you have this, you must complete a more detailed discharge letter/summary using a proforma that you will be provided by Dr Hullamane on your first day. Once this is completed, you must email it to Donna, the secretary, who then send it to the patient’s GP.
Admitting Acute Admissions
At any point in the day, you may get bleeped to clerk in an acute admission for a patient falling under Dr Hullamane’s care. It is helpful to get a handover from the Psychiatric Liaison Team who usually sees the patient first in A+E prior to bringing the patient to Bushey Fields. Before seeing the patient, ensure you have a purple clerking booklet, drug chart (to write regular medications on), capacity assessment form, cardiometabolic form and care cluster form.
You must also complete respiratory / cardiovascular / neurological examinations and document these findings. Once this is done, you must obtain a baseline ECG for the patient, with their consent, as some psychotropic medications can affect QTc intervals. Take your time when clerking and try to cover all the headings in as much detail as possible. NB: you will always have a nursing colleague present during the clerking session.
MHAS clinic
Wednesdays consist of assessing patients referred to MHAS (Mental Health Assessment Clinic) which is where psychiatrists assess patients referred by local GPs. You will be given one patient per week and this involves taking a full psychiatric history and mental state exam, formulating a provisional diagnosis and making the next plan of action. This may involve considering urgent inpatient admission, adjusting/starting medications or signposting to other services for support such as drug and alcohol services/bereavement support/AA etc. Afterwards, you will be required to fill in a detailed report. This is a great learning opportunity to use diagnostic skills and formulate management plans safely under the guidance of Dr Byra-Reddy or Dr Hullamane.
Ward work
Ward work involves answering bleeps about any patient concerns regarding physical health issues such as new-onset cough/chest pain/skin infections/cellulitis etc. You may also get bleeped to speak to an agitated/suicidal patient who may be wanting to leave the ward or have their section 17 leave amended. Some of these situations can be overwhelming/challenging, but it is important to not make any decisions about patient’s leave entitlements without speaking to a senior member of the team. Sometimes patients sadly take overdoses of ibuprofen/paracetamol/other medications
– which requires urgent bloods to measure paracetamol levels and LFTs, and/or transfer to A+E for treatment with NAC. Toxbase is a good resource to refer to when interpreting paracetamol/drug overdose levels (the password can be found in the Dr’s office in Rowans). Finally, as ward rounds take place once a week, it’s a good idea to catch up with how patients are doing daily by reading the medical/nursing notes to keep up to date with how they are progressing.
Early Intervention Psychiatry
Zoning
This takes place every morning at 9:30am at Cross Street Health Centre. It is chaired by the Duty Worker for the day who is on call (checks various items, receives the referrals and deals with the days general enquiries). This rotates between the Care Coordinators. During the meeting Care Coordinators can discuss their patients if they have any concerns and feedback to the team for advice. This is also an opportunity for initial assessments of referrals to be fed back to the team and opportunity to decide whether or not they are suitable for the service.
Patients are classified in order of risk. Therefore, patients in secure or inpatient settings are discussed first; red (seen or spoken to at least twice a week), amber and green.
On a Tuesday the meeting begins at 9am and is a longer meeting. You may get to this if RHH teaching is cancelled. It can be a business meeting, clinical meeting or case conferences can be held for patients among other things.

Ward Reviews
Take place on a Thursday, 14:00 onwards. You must gather the patient’s notes, drug charts and find out from the nursing team how the patient has been over the weekend. You can find designated ward round proforma sheets in the top shelf of the filing cabinets in the main ward office. Document clearly who is present (sometimes a variety of health and social care professionals may attend the ward round) and be sure to fill in the Mental State Exam section and note any medication changes. If patients need Section 17 leave forms (blue), you can find these in the top drawer of the filing cabinet in the main office.

Work with the EI team
Early Intervention is a secondary service based in the community, set up in 2005. They take on patients who have had suspected first episode of psychosis or ‘At Risk’ of developing a first episode of Psychosis (aged 14-65 years old). Therefore, patients are classified as FEP (First Episode Psychosis) or ARMS (At Risk Mental State). The team is made up of various members of the multidisciplinary team in order to facilitate a holistic approach. This team includes: medics, CPNs, social worker, OT (occupational therapist), STR (Support Treatment and Recovery) and psychologists. Your role as the junior doctor on the team includes being involved in ward reviews, CPAs, writing discharge summaries, clinic letters and GP letters re physical health. In addition, you will run the physical health clinic, which includes monitoring bloods and taking action if required
Discharge Letters
Once an inpatient has been discharged from BFH, it is your duty to write to the GP. The team will be sent the inpatient notes. It is really important to make this as detailed as possible as this becomes a good reference for future clinics. So, utilise your resources: inpatient notes, outpatient notes, previous clinic letters and OASIS. Get in your head a timeline of events and services the patient has engaged with. A template will be available.
Annual leave
You can choose when you have your zero day as in either the Monday or the Friday after working a weekend. Make sure the secretary is aware.
You are not required to find junior doctor cover for your annual leave so it should be reasonably flexible. There is a form that needs to be filled in and be signed by Dr Ravi. A copy needs to go the postgraduate coordinator who is based at the Henry Lautch Centre.
Physical Health Clinic
This clinic will run every second week. This clinic will be done with yourself and one of the CPNs, appointments last 45 minutes. This will involve enquiring about lifestyle, taking necessary bloods, ECG and other measurements. It is your responsibility to chase the blood results and liaise with the GP accordingly if there were any abnormalities.
Psychiatry Learning Opportunities
for Old Age:
Try and attend the MDT at Woodside, it’s a nice time off the ward and also a chance to hear interesting patient cases from the community.
For General Adult Psychiatry:
Try to attend an ECT suite session (email Dr Iqbal/his secretary) as it is a unique opportunity to witness and assist in a non-pharmacological treatment for severe depression/mania/catatonia. It’s also a great opportunity to shadow any Psychiatry Core Trainee doctors doing clinics at Halesview Community Mental Health Service in Halesowen, as you see a variety of psychiatric presentations and get a better understanding of what it is like to be a psychiatrist when not in acute ward settings.
For Ei Psychiatry:
During the rotation, if time permits, observing some of the following will be very useful for learning and reflection.
- Observe a tribunal (contact the MHA office at HLC)
- Observe CAMHS consultant lead clinic at Cross street on a Wednesday
- Observe psychologists’ work
- Improve teaching abilities by teaching the students on placement with EI

General Opportunities
- Balint group happens every Friday morning and is a lovely way to make sure you don’t become emotionally burnt out, use your cases for your reflection on your portfolio too!
- Make sure you do an audit during psychiatry; you can rent a book from the psych library (101 psychiatry audit ideas – the librarian will help you find it) or do one with your consultant as it is a nice rotation to take your time with.
- Grand Rounds are weekly on Thursdays between 1300-1400 in the education centre. These are lectures presented by different clinicians in the trust on useful and important.
- It’s a good idea to catch up with any script modules that you have pending during any spare time in between ward work to meet the portfolio.
Useful Topics to Revise
- Psychiatric History Taking for depression / anxiety / psychosis / schizophrenia
- Mental State Examination
- Alcohol History Taking
- Suicidal History Taking
- Psychotropic medications/Antidepressants/Anxiolytics (especially side effects/ overdose symptoms)
- Mental Health Act g.:
- Section 5(2),
- Section 2,
- Section 3,
- Section 17
- Personality Disorders