Respiratory Medicine induction booklet was contributed by the following;
written by Dr Ganesh Rajaratnam
reviewed by Dr Manish Pagaria
updated by Dr Hamzah Rafiq
Select the booklet titles below to expand the table to view more information.
Respiratory Ward Timetable
| Day | Monday | Tuesday | Wednesday | Thursday | Friday |
|---|---|---|---|---|---|
|
AM |
Ward |
FY1 Teaching |
Ward |
Ward |
Ward |
|
PM |
Lung MDT Ward |
Ward-based Teaching / Ward |
Ward |
Ward |
X-Ray Meeting |
Consultants ward round table
| Day | AM - Ward Round | Lunchtime Meeting ( Education Centre) | PM - Ward Round |
|---|---|---|---|
|
MONDAY |
Dr Brammer |
Lung Cancer MDT Meeting |
Dr Chaudri |
|
TUESDAY |
Dr Pagaria |
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
Grand Round |
Dr Chaudri |
|
FRIDAY |
Dr Pagaria |
Radiology Meeting |
|
Every morning a respiratory DRAS Ward Round is done on AMU Note: The consultants do not necessarily follow this timetable and most of them will be on the ward daily. Consultants are easily contactable on their personal mobiles via switchboard should you have any questions about patients that are under them.
Respiratory Medicine Ward
Patients on the Ward
The respiratory ward is a 4-station medical specialty ward. Each junior is assigned to a station and ideally you will cover this station all week so you become familiar with the patients. You may sometimes have to change stations depending on staffing levels.
Respiratory Team
The respiratory team is currently made up of 7 consultants, 3 registrars, 6 SHOs, and an FY1. The entire team are very helpful, and don’t feel hesitant to ask for help as everyone is willing to teach and help out.
There is a team meeting with a consultant present every Monday at 09:00 in the doctor’s office on ward to ensure there are enough junior doctors on the ward and they are assigned to a station. Discussions about clinic attendance during the week also take place during this meeting. Usually there will be one junior per station (12 patients), although sometimes there may be 2 of you.
Ward Rounds
There is a timetable for the Consultant ward rounds, but most of them will come daily to the ward to review their patients (especially the sick ones). Consultants will see their own patients – these are the patients who are admitted while that consultant is on call, or any long-term patients who see that consultant regularly. However not every consultant will be on the ward every day. It is your responsibility to ensure every patient on your station is reviewed every day, which means patients who aren’t seen by their parent consultant will need to be seen by you. If you don’t feel comfortable doing this initially, just let one of your seniors know so they can help. See later in the handbook for a guide to running your own ward round.
Ward Duties
After the rounds, you will need to complete your jobs. If there are two of you on the station, then split the jobs and work efficiently to get them done. Remember, you can always ask for help if you need. Prioritise urgent jobs such as arranging scans, and seeking other speciality reviews ahead of less urgent jobs such as reviewing routine bloods which often come back by the afternoon.
Pharmacists
The registrars or consultants (2nd port of call) are often around to help, and are more than happy to be bleeped/called. They are particularly useful when you have sick patients that need reviewing, questions about changing NIV settings or titrating O2 etc.
On respiratory you have a brilliant pharmacist. Hassan will help out with most of the TTOs. At the end of your rounds, work out who needs TTOs, after completing, inform the ward pharmacist and nursing team. Remember this isn’t actually his job, so treat him with respect. Check if he actually has time to do your TTO, don’t just assume he does. Pharmacists are also very useful in answering any questions you have about medications or being able to find what a patient’s regular medications at home may be, if the patient doesn’t know or doesn’t have their prescription sheet with them.
Respiratory - Undertaking your on Ward Round
Dr Michael (orthogeriatric consultant) has a specific way that he likes the ward round to be documented.
A useful Ward Round Checklist
-
1.
A brief up-to-date description of admission complaints and current issues.
-
2.
Recent Observations - always check for temperature spikes in the last 24 hours, and useful to look at what a patient’s oxygen saturations have been, i.e. are they in the target range?
-
3.
Recent Blood results, if bloods have been taken within 24 hours you can always call biochemistry via switch to add tests such as: TSH, magnesium, B12 & Folate. Particularly useful if patients are difficult to bleed.
-
4.
Post-op complications and whether they have resolved
-
5.
Recent imaging findings. (You aren’t expected to interpret CT images, but things like CXR you are. Again, if ever unsure check with the team). Always read the reports and pick up on any abnormal findings, often the ‘conclusion’ part helps to highlight the significant findings. Make sure to document scan results once you’ve reviewed them.
-
6.
Any acute medication they’re currently on, such as antibiotics and whether these are IV or oral. When are they due to finish? Can the patient be switched to oral antibiotics?
Specialty Specific Documentations
Chest drain
In patients with chest drain for pleural effusion, always document the total amount of fluid drained and also the amount of fluid drained in the last 24 hours. This helps to make decisions regarding removal of the drain. Also document the physical appearance of the fluid. In patients with chest drain for pneumothorax, look for bubbling or swinging of the chest drain on deep breathing or coughing and document that.
Patients on NIV
Document the settings on the machine (IPAP and EPAP), duration of NIV used in the last 24 hours and also the number of days patient has been on NIV.
ABG
While documenting ABG it is very important to document the FiO2 (if on venturi mask) or the flow rate (on nasal specs). Do not forget to mention if ABG was done on NIV or how long after the patient came off NIV. If you have changed the amount of oxygen being delivered to a patient it is worth waiting around ten minutes for the patient to adjust to the new amount before doing the ABG. This will allow for more accurate results.
Oxygen
Please ensure that oxygen is prescribed for all patients with a target saturation range. If unsure what their target range should be, ask a senior. For example, not all patiReents with COPD will have a target saturation range of 88-92%.
Microbiology
Check and document current and previous sputum culture results and sensitivities as it will help to decide the right antibiotic and duration of treatment.
"Ask the patient about symptoms to do with their current admission i.e. a detailed respiratory history."
- Worsening SOB – sudden or not
- Cough – productive? Haemoptysis? Volume and colour of phlegm
- Chest pain – full SOCRATES if indicated
- SOBOE
- Orthopnoea / PND
- Any leg pain or swelling
Systems review:
- Neuro symptoms
- CV – chest pain, palpitations, BP
- GI – pain, Bowels, vomiting
- GU – dysuria, haematuria, output
- MSK – pain
- Are they eating and drinking?
- Have they passed urine? Is there a catheter in situ?
- When’s the last time they opened their bowels, is this normal for them?
Examination:
- General appearance
- Pulse
- JVP
- Listen to the chest
- Heart sounds
- Abdo exam
- Calves/peripheral oedema.
When looking at observations, respiratory patients will often score highly as their baseline (A CO2 retainer on O2, will immediately score at least 3). Therefore, it is always important to look at trends, especially when looking at saturations.
Remember, they are not looking for you to be a respiratory consultant; you are there to pick out the deteriorating patient, red flags and monitor treatment.
This may sound like a lot to cover but as you become more experienced you will become more efficient and faster. The above is my tips on how to do a ward round, but as you do more you will develop your own method that suits you.
Respiratory - Common jobs on ward C5
Common jobs
After you’ve seen all the patients, you will spend the rest of the day doing ward jobs. These will usually be generated during your ward round, but some things like cannulas can come up at any time during the day. It is important to keep a list of jobs so you remember what needs doing and so you can prioritise tasks. It’s also satisfying to cross them off once you’ve done them! I like to use a piece of paper, write the bed numbers and patient initials, then write jobs for the patients as I go along, with an unfilled box. Once the job is completed you can fill the box in, the ultimate feeling of satisfaction.
Remember, they are not looking for you to be a respiratory consultant; you are there to pick out the deteriorating patient, red flags and monitor treatment.
This may sound like a lot to cover but as you become more experienced you will become more efficient and faster. The above is my tips on how to do a ward round, but as you do more you will develop your own method that suits you.
Common jobs on C5 include:
Select the titles in red below to find out further information.
This is a skill you will get very good at while working on C5. ABGs are very useful for monitoring patient progress when they are admitted with respiratory failure. Patients who are on NIV will need regular ABGs, often 3 or 4 per day – the nurses can often help you out if there are lots to do.
Sometimes a patient will need to go home on LTOT (Long Term Oxygen Therapy). These patients need ABGs on room air and on whatever oxygen they are going home with.
Cannulas are for patients requiring IV antibiotics and/or IV fluids.
Patients going for contrast CT scans will also require a cannula (green or above). Most other patients will be fine with a pink or a blue.
Make sure you order bloods before you go home for the patients who need them the next morning. In that case the phlebotomists will usually do them all for you. Sometimes though, the phlebotomists won’t come, or they won’t be able to bleed a patient and it will be up to you to do it. The same applies to new patients who arrive on the ward overnight or anyone you forgot to order for.
You will need to follow up the results and act on anything abnormal. You can make order sets on Sunrise and these are very useful with ordering the common blood tests. These include renal profile, bone profile, liver profile, full blood count and CRP.
C5 patients often have significant comorbidities, and they sometimes need input from other specialty teams. Contact the switchboard and ask for the bleep of the on-call registrar for the specialty you need.
Be prepared with an SBAR-style handover when you talk to the reg. You can use the latest ward round entry and order sheet on Sunrise to help dictate the conversation. Don’t feel bad if they ask you some questions you can’t answer, but try to at least know why you are phoning them and what you would like them to do.
This will be something that you won’t feel confident doing at first. Try to observe the consultants and registrars speaking to family members and pick up on the techniques they use. Establish whether the relative is next of kin and try to get permission of the patient to update the relative if possible.
It’s always a good start to ask what they’re understanding of the situation is thus far. This helps guide the conversation and allows you to understand what the relative knows so far.
As mentioned above, Hassan, the pharmacist will often be around to help do most of the TTOs for you. However, you will still need to do some yourself. Try to include all the relevant information from the admission. Think to yourself: “If I were a GP what would I want to know about this person’s admission?”
Or imagine you are the doctor clerking that patient next time they come to ED. “What information would be helpful?” This includes results of significant investigations, any outpatient follow-up or investigations that are scheduled.
Furthermore, has there been any medication changes to what the patient took pre-admission (i.e. anti-hypertensives stopped due to postural hypotension and for the GP to review whether to recommence).
Currently, there are discharge doctors working across the hospital who can help do the TTOs, (you can put TTOs needed on Nerve Centre), but make sure to put them on early in the day. In case they aren’t able to and you’ll have to try to do the TTO in the afternoon. Prioritise TTOs of patients that may go the same day.
Respiratory - Further Information
Respiratory Medicine during the COVID Pandemic
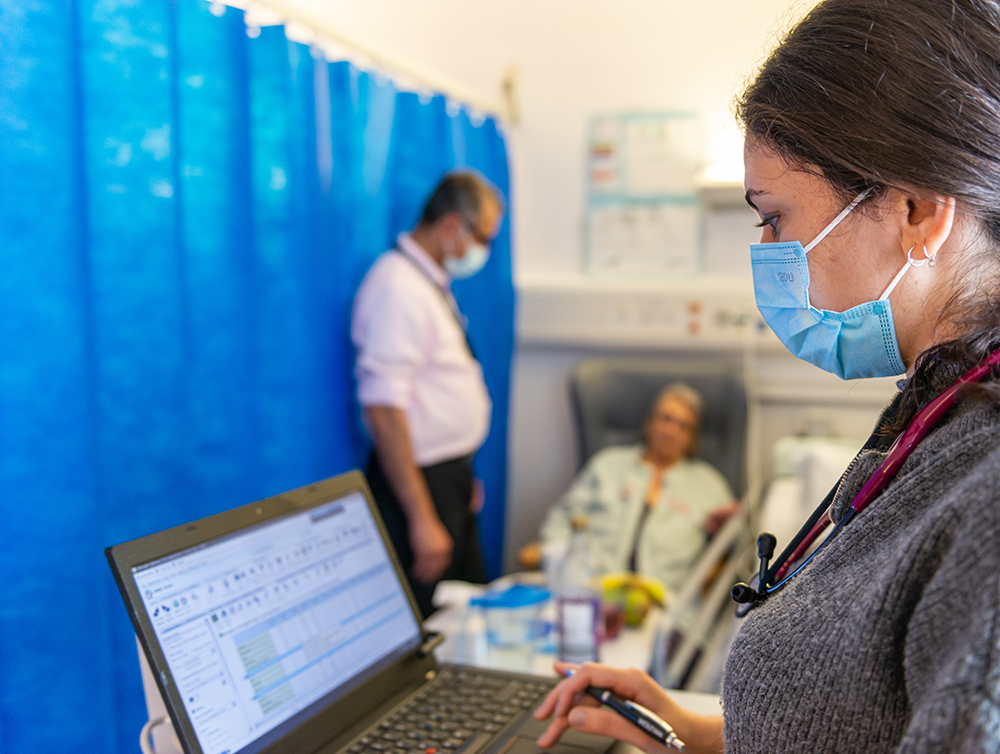
Depending on how much COVID19 is still affecting the wards, your experience on C5 may differ slightly from what you have read so far. As of May 2020, C5 is an Isolation Ward, with certain stations specifically designated for COVID-positive patients. Staff on the ward are required to wear a protective face mask at all times, and when directly interacting with patients you are also required to wear an apron and gloves.
Consultants are more present on the wards, with 1 consultant covering 2 stations and all patients being seen by a consultant or registrar every day. As the pandemic starts to die down, it is likely the ward will revert back to normal, but there may still be parts of the ward where special precautions are required.
Bereavement
- While working on respiratory it is inevitable that some of your patients will reach the end of their lives. This is especially true if you are on respiratory during the winter months.
- Ensure you are familiar with the process of verifying a death. This is a skill you will have to use at some point whether it is on C5 or during your on-calls. There is an excellent guide available on GeekyMedics.
- When a patient whose care you were involved in dies, you may be asked to write their death certificate down in the bereavement office. The team there is very helpful and will help you fill out the necessary forms. Before you go down, try to discuss the patient with their parent consultant so you know what to put as the cause of death.
- It is good practice to also document the cause of death in the notes in the same format as the death certificate.
- It is natural to be emotionally affected by the death of one of your patients. Don’t be afraid to talk to your educational or clinical supervisor if you feel you need support. The respiratory consultants are all very friendly and will be willing to help you too.
Learning Opportunities
The MDTs are useful to attend, in order to get a general feel of how they work. Don’t be afraid to ask questions. If you don’t feel comfortable whilst the meeting is happening, note down patient details and ask the questions after.
There are always a lot of audits to be undertaken in respiratory and Dr Pagaria is a useful person to get in contact with, if you desire to do so.
There is scope to get a lot of hands-on experience on respiratory. The best way to do this is to let the registrars know you are interested, as they perform a lot of the pleural procedures, not only for the respiratory ward, but also the rest of the hospital.
There are a multitude of practical skills that you can get involved in. Things you should gain experience in include:
- Chest drain removal – this is something you will be able to do by yourself by the end of the rotation
- Pleural aspiration
- Chest drain insertion
- Chest drain management
- NIV management
Health and Wellbeing
Staff that are happy and thriving in their working environment will inevitably have a more enjoyable experience in the workplace, contributing to the provision of excellent health care for all of our patients. The Dudley Group recognises our commitment to staff wellbeing in a variety of ways.
Select the link below to find out more how the Trust can support you.